


Pharmaceutical R&D leaders face a stark execution gap. You've piloted decentralized trials, invested in AI-driven site selection, and explored real-world evidence. Your strategy acknowledges the need for transformation. Yet, 68% of digital health pilots never move beyond the test phase, and clinical trials face similar scaling challenges.
The difference isn't ambition; it's operational discipline. While most companies cycle through endless pilots, leading organizations are achieving measurable transformation. AI-driven site selection and process improvements compress development timelines by six months per asset and reduce concept-to-first-in-human cycle time by 40%. Contract lifecycle automation cuts investigator onboarding by 50%, reducing oncology study timelines from 120 to 60 days. These improvements boost enrollment by 10-20% and improve top-enrolling site identification by 30-50%.
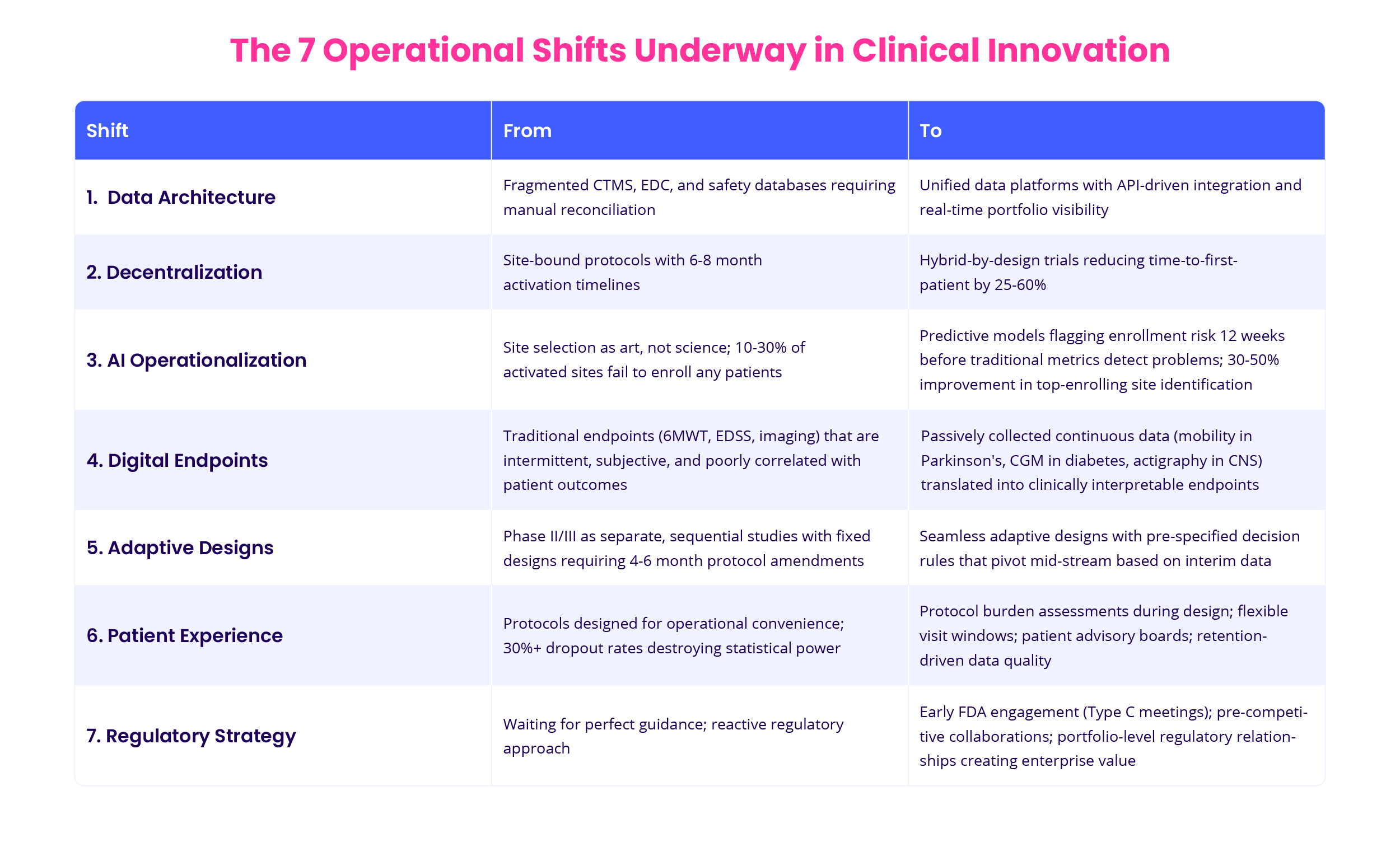
Exhibit 1: The 7 Operational Shifts Underway in Clinical Innovation
The gap is widening. Companies that can't operationalize the shifts within 24 months will miss compounding benefits in timelines, costs, and competitive positioning. This article determines the seven operational shifts that separate leaders from followers and the implementation roadmap to close the gap.
This article breaks down:
-
The seven operational shifts separating leaders from followers (from unified data architecture to proactive regulatory strategy)
-
What actually failed before these companies succeeded (30% higher protocol deviations, 3x longer onboarding times, FDA pushback on data quality)
-
Honest ROI calculations: $18-43M investment, 18-24 month breakeven, and why pilot-only strategies never generate returns
-
The implementation roadmap for moving from fragmented systems to portfolio-wide transformation
Understanding clinical innovation today
The industry has moved beyond isolated digital tools to integrated clinical research ecosystems where discovery, development, and evidence generation operate as a connected system, not sequential handoffs.
What's changed at leading organizations:
-
From fragmented CTMS, EDC, and safety databases requiring manual reconciliation
to unified data platforms with API-driven integration and real-time portfolio visibility -
From site-bound protocols with 6-8 month activation timelines to hybrid-by-design trials, reducing time-to-first-patient by 25-60%
-
From reactive monitoring, flagging issues after delays compound
to predictive analytics identifying enrollment risk 12 weeks before traditional metrics detect problems -
From phase II/III as separate, sequential studies to seamless adaptive designs that pivot mid-stream based on interim data
Organizations like Roche, Novartis, and Eli Lilly are embedding them into portfolio strategy, regulatory frameworks, and operational SOPs. The result: measurably faster timelines, lower attrition, and portfolio capacity increases of 20-30%.
The evolving role of clinical research in treatment development: From cost center to strategic engine
Clinical research becomes a bidirectional system: feeding real-time insights back into early-stage R&D decisions and forward into post-market evidence generation.
Leading companies now use clinical operations as a continuous learning engine, not a series of discrete studies:
-
External control arms replace randomization in rare biomarker populations, accelerating market access by more than one year (Roche/Flatiron in NSCLC)
-
Adaptive designs enable mid-trial pivots based on interim studies, eliminating rigid phase boundaries
-
Real-world evidence platforms supplement trial studies for label expansions, reducing the need for additional RCTs
The result: clinical research generates compound value. Each study builds regulatory precedent, operational learnings, and evidence infrastructure that accelerates subsequent programs.
The operational implication: Companies that still treat clinical as a "run the protocol" function are leaving 20-30% portfolio capacity on the table.
Clinical trials as the engine of treatment development: The end of "One and done"
Clinical trials are no longer discrete studies with fixed endpoints; they're becoming continuous learning systems that generate evidence across multiple stakeholder groups simultaneously.

Exhibit 2: How each trial becomes a multi-purpose asset
The traditional model treated trials as pass/fail gates: run the protocol, lock the database, submit. That linear approach is breaking down. Modern trials now serve multiple objectives in parallel:
-
Regulators expect real-world performance studies and biomarker validation alongside safety/efficacy
-
Payers demand cost-effectiveness analyses and real-world adherence studies beyond clinical endpoints
-
Physicians need subgroup-specific responses and predictive biomarkers, not just dosing guidelines
-
Patients benefit from burden-optimized protocols and remote access, not just investigational therapy access
This shift is enabled by hybrid and decentralized models integrating eConsent, telehealth, and wearables, creating infrastructure for richer, more diverse datasets that answer questions beyond the primary endpoint.
The operational implication: Each trial becomes a multi-purpose asset. Your phase III oncology study simultaneously generates efficacy data for approval, real-world evidence for payers, and validated biomarkers for patient selection.
The result: Clinical development evolves from binary checkpoints to a connected evidence generation engine, where each study compounds learning for the next.
Patient experience drives clinical studies' quality and commercial success
The connection is direct: patient dropout destroys statistical power and introduces bias. At 30%+ attrition rates, you're not just losing study points, you're compromising the validity of your entire endpoint analysis.
The business case for human-centric design:
-
Higher retention = cleaner data: Janssen's Heartline Study achieved notably higher retention than typical cardiology trials by eliminating mandatory site visits and using app-based engagement, demonstrating that patient-centric design directly impacts data quality.
-
Better adherence = real-world validity: Trials conducted around patient realities generate evidence that translates to post-market performance, reducing payer pushback and prior authorization barriers.
-
Diverse participation = broader labels: Decentralized models have demonstrated improvements in diversity metrics, with Novartis reporting that remote participation enabled broader enrollment from wider community and socioeconomic backgrounds, supporting more inclusive approved populations.
Modern protocols embed patient-reported outcomes, wearable-captured behavioral data, and quality-of-life metrics, not as exploratory endpoints, but as co-primary measures. The result: treatments that perform in clinical practice, not just controlled trials.
The tension: Your medical monitors will resist protocol flexibility, viewing it as compromising scientific rigor. The data shows otherwise: Patient burden is a data quality issue, not a convenience issue.
Why most "innovation" initiatives fail in clinical development
R&D leaders understand the theoretical value of decentralized trials, AI-driven site selection, and real-world evidence. The core challenge is execution against entrenched constraints:
-
Legacy system paralysis: Your CTMS, EDC, and safety databases don't communicate. Integration projects take 12-18 months and still require manual reconciliation.
-
Risk-averse culture: Medical monitors and CRAs trained on traditional models resist protocol flexibility. "We've never done it that way" remains the most expensive phrase in clinical operations.
-
Regulatory ambiguity: FDA guidance on digital endpoints exists, but operationalizing it requires navigating Division-specific interpretations and building validation frameworks your statisticians don't yet trust.
-
Vendor fragmentation: You're managing 15+ point solutions across patient recruitment, ePRO, wearables, and data management. None were designed to interoperate.
The result? Pilot studies that never scale. Innovation theater that doesn't reduce cycle times or create new medications.
The seven operational shifts that separate clinical research and clinical trial leaders from followers
Clinical research is undergoing structural transformation. From site models to data architecture, a new operating model is emerging. One that prioritizes speed, flexibility, and evidence generation at scale.
These seven shifts reflect the strategic retooling of how clinical trials and clinical studies are designed, executed, and connected to treatment development. Companies that can't operationalize these shifts within 24 months will face increasing pressure on timelines, costs, and portfolio productivity.

Exhibit 3: The effect of applying the shifts on time-to-impact
Shift 1: From point solutions to enterprise data architecture
The problem you're solving: Fragmented systems create data latency, reconciliation burden, and single-source-of-truth conflicts that delay decision-making by weeks per milestone.
What good looks like: A unified clinical data platform where CTMS, EDC, safety databases, and biomarker systems share normalized data models. Real-time dashboards that don't require weekend data pulls. API-driven integration that eliminates manual exports.
Why it's hard: This requires deprecating systems with vocal stakeholders, negotiating enterprise licenses, and accepting 6-12 months of parallel operations during migration. Most organizations lack the executive sponsorship to force this through.
ROI reality check: Organizations implementing unified clinical data platforms report significant improvements in data management efficiency. Industry studies show EDC systems can reduce query rates by up to 70% and decrease time to database lock by up to 45%. Automation of data workflows reduces manual effort by 30-40%. However, implementation requires substantial investment in technology infrastructure and organizational change management, with enterprise-scale deployments typically requiring 6-12 months of parallel operations during migration.
Shift 2: Decentralization as default, not exception
The problem you're solving: Traditional site models create geographic bottlenecks, limit diversity, and drive 25-35% dropout rates due to visit burden.
What good looks like: Hybrid-by-design protocols where every visit is evaluated for decentralization potential. Pre-negotiated home health networks. Mobile phlebotomy and imaging partnerships. ePRO systems that don't require patient training calls.
Why it's hard: Your CRAs don't know how to monitor decentralized visits. Medical monitors worry about data quality without direct observation. Legal teams flag liability concerns for home-based assessments. Budgets don't accommodate higher per-patient costs upfront (even when total costs decrease through better retention).
What actually moves the needle: Decentralized trial models have demonstrated operational viability in reducing patient burden, though specific enrollment and retention improvements vary by therapeutic area, protocol design, and operational maturity. Organizations like Roche and Novartis have piloted decentralized approaches in oncology and neuroscience, requiring 9-12 months of operational redesign, new monitoring SOPs, and multiple pilot iterations to refine the model before achieving consistent results.
The catch: Decentralization increases per-patient costs by 15-20% in phase II but reduces overall program costs through faster enrollment and lower dropout penalties. Finance teams often kill these initiatives by focusing on the wrong metrics.
Shift 3: AI operationalization (beyond vendor promises)
The problem you’re solving: Site selection remains art, not science. Industry data shows 10-30% of activated sites fail to enroll any patients, while top-enrolling sites outperform median sites by 2-4x. You're burning 6-8 weeks per protocol, negotiating feasibility with sites that will underperform.
What good looks like: Predictive models trained on historical enrollment performance, PI publication history, site infrastructure, and patient catchment data. Probabilistic forecasting that flags enrollment risk 12 weeks before slippage becomes visible in traditional metrics. Investigators and researchers play a key role in interpreting predictive models and ensuring that site selection aligns with trial protocols and participant safety.
Why it’s hard: Most “AI-powered” vendors provide black-box scores without auditability and interventions. Your biostatisticians won’t accept predictions they can’t validate. Training data is biased toward past site relationships, perpetuating inefficiencies. Model outputs require human interpretation; they don’t make decisions for you. Investigators are often required to validate AI-driven site selection outputs and ensure compliance with regulatory standards.
What’s working now: Industry analysis shows AI-driven site selection improves identification of top-enrolling sites by 30-50% and accelerates enrollment by 10-15% across therapeutic areas. Companies implementing AI/ML in clinical operations report an average 18% time reduction. The key to success isn't the algorithm—it's integrating predictive outputs into existing feasibility workflows and training clinical trial managers to interpret probabilistic outputs.
Reality check: AI won’t fix bad protocol design or unrealistic inclusion criteria. It accelerates good decisions; it doesn’t compensate for strategic mistakes.
Shift 4: Digital endpoints - navigating validation without waiting for perfect guidance
The problem you’re solving: Traditional endpoints (6MWT, EDSS, imaging) are intermittent, subjective, and poorly correlated with patient-relevant outcomes. Wearables and sensors can capture continuous, objective data, if you can validate them.
What good looks like: Passively collected mobility data in Parkinson’s. Continuous glucose monitoring in diabetes bridging studies. Actigraphy replacing sleep diaries in CNS trials. Algorithms that translate raw sensor data into clinically interpretable endpoints.
Why it’s hard: FDA’s CDER guidance on digital health technologies is framework-level, not prescriptive. You need therapeutic-area-specific validation strategies. Regulatory agencies, including the federal government, require enough information in clinical trial applications to approve the use of digital endpoints and ensure participant safety. Endpoint adjudication requires new statistical methods your DMC may not accept. Device management (provisioning, compliance monitoring, data transfer) is operationally complex.
Where leaders are winning: Biogen validated smartphone-based gait metrics in MS trials by running parallel traditional assessments and demonstrating correlation. This took 18 months longer than anticipated, but created a reusable framework. Eli Lilly is embedding continuous glucose monitors in phase II diabetes trials, not as exploratory endpoints, but as co-primary measures, accepting regulatory risk to build first-mover evidence.
The trade-off: Early adoption means longer regulatory discussions and potential Phase III redesign if endpoints don’t hold. Late adoption means competitors establish precedent without you.
Shift 5: Adaptive designs (when they're worth the complexity)
The problem you’re solving: Traditional phase II/III boundaries waste time and expose patients to ineffective doses. Fixed designs can’t respond to interim signals without protocol amendments that add 4-6 months.
What good looks like: Seamless phase II/III transitions with pre-specified decision rules. Platform trials testing multiple assets against shared infrastructure. Bayesian designs that accumulate evidence continuously rather than waiting for arbitrary enrollment milestones.
Why it’s hard: Adaptive designs require upfront statistical investment that delays study startup. Regulatory submissions are more complex. Data monitoring committees need different expertise. Operational systems (randomization, drug supply) must handle dynamic allocation.
When it works: Small patient populations (rare diseases), oncology biomarker-selected subgroups, and settings where rapid dose optimization matters (antivirals, vaccines). Master protocols in oncology (I-SPY, LUNG-MAP) reduced per-asset development time by 30-40%, but required consortium governance that most organizations can’t replicate internally.
When it doesn’t: Large indication trials with stable standard of care and predictable enrollment. The operational complexity doesn’t justify marginal time savings.
When an adaptive trial ends, data analysis is conducted, results are reported to regulatory agencies, and participants are informed about the outcomes and next steps.
Shift 6: Patient experience as a quality metric
The problem you’re solving: Dropout rates of 30%+ destroy statistical power and introduce bias. Patients drop out because protocols are designed for operational convenience, not human beings.
What good looks like: Protocol burden assessments during design (not after IRB approval). Patient advisory boards reviewing visit schedules and procedures. Doctors are involved in reviewing protocols to ensure that the medicine being tested aligns with patient needs and safety requirements. Simplified consent documents tested for comprehension. Flexible visit windows that accommodate work schedules.
Why it’s hard: Your medical team prioritizes scientific rigor over patient convenience. Flexibility is perceived as compromising data quality. Burden assessment tools don’t yet have industry-standard frameworks. Sponsors fear that “making trials easier” signals lower scientific standards to regulators.
Evidence base: Janssen's Heartline study demonstrated sustained high participant adherence through 2-year follow-up by designing around participant convenience: app-based engagement, no mandatory site visits, wearable-driven data capture. The study enrolled over 34,000 participants, representing one of the largest decentralized cardiovascular trials. But this model doesn't translate to phase III oncology trials requiring frequent imaging and lab assessments.
The real challenge: Balancing patient burden with data quality requirements. There’s no universal answer. It’s indication-specific and requires trade-offs your clinical team must consciously make.
Shift 7: Regulatory strategy as competitive differentiator
The problem you’re solving: Regulatory pathways for digital tools, real-world evidence, and novel endpoints are negotiable, but most sponsors wait for perfect guidance before moving.
What good looks like: Early engagement with FDA (Type C meetings) to align on digital endpoint validation plans. Pre-competitive collaborations (Critical Path Institute, TransCelerate) to establish measurement standards. Regulatory CMC plans that incorporate continuous learning from phase II into phase III without triggering Major Amendment risk. The federal government provides resources and oversight to ensure that clinical research meets safety and ethical standards, supporting sponsors with guidance and informational materials.
Why it’s hard: Regulatory affairs teams are trained to minimize risk, not optimize time-to-approval. Early FDA meetings require well-formed positions, which you don’t have until you’ve piloted the approach. Division-specific interpretations vary; what CDER accepts, CBER may question.
What’s working: Roche’s use of Flatiron Health’s real-world data for external control arms in oncology wasn’t approved by precedent. It was negotiated through structured dialogue and methodological rigor. This created regulatory precedent that competitors now leverage.
The insight: Regulatory strategy is portfolio-level, not study-level. Organizations that build regulatory relationships around methodological innovation (not specific assets) create enterprise value that compounds across programs.
Three case studies showing clinical trial innovation lessons
Top pharmaceutical companies are reshaping how clinical trials are designed, executed, and scaled.
The focus is shifting from site-bound, sequential studies toward flexible, technology-enabled models that accelerate learning, expand access, and improve patient care. These innovations are strategic levers to reduce timelines, improve safety, and increase the probability that a new drug will be successfully approved.
By rethinking how research participants engage with studies, how data is captured, and how different trials can run in parallel, these companies are redefining what modern, adaptive clinical development looks like.
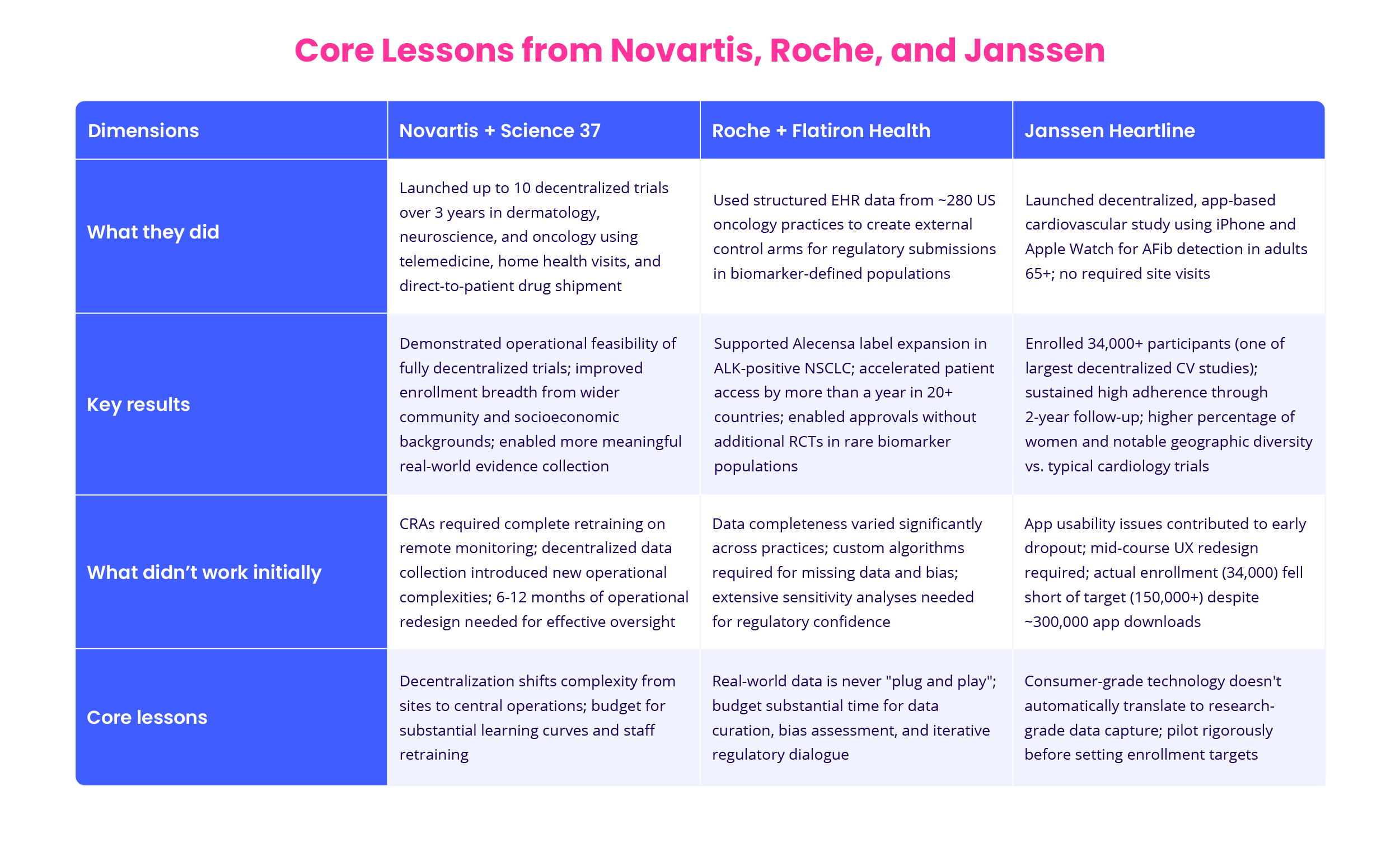
Exhibit 4: Core Lessons from Novartis, Roche, and Janssen
Novartis + Science 37: Decentralization in neuroscience
What they did: Partnered to launch up to 10 decentralized clinical trials over three years in dermatology, neuroscience, and oncology using telemedicine, home health visits, and direct-to-patient drug shipment through Science 37's NORA® platform. The decentralized model enabled participants to engage from home, expanding access beyond traditional site-bound trials.
Results: The partnership demonstrated the operational feasibility of fully decentralized trials in therapeutic areas traditionally reliant on frequent site visits. Novartis reported that remote participation improved the breadth of enrollment from wider community and socioeconomic backgrounds while enabling more meaningful real-world evidence collection.
What didn't work initially: CRAs required complete retraining on remote monitoring protocols. Decentralized data collection introduced new operational complexities around protocol compliance and monitoring SOPs that weren't present in site-based trials. The partnership necessitated 6-12 months of operational redesign to establish effective oversight of remotely-collected data.
Lesson: Decentralization isn't operationally simpler. It shifts complexity from sites to central operations. Budget for substantial learning curves, operational redesign, and staff retraining when moving beyond pilots.
Roche/Genentech + Flatiron Health: Real-world control arms
What they did: Used structured electronic health record (EHR) data from approximately 280 US oncology practices within Flatiron Health's network to create external control arms for regulatory submissions. This approach enabled label expansions in biomarker-defined populations without requiring additional randomized controlled trials.
Results: Supported regulatory approval for Alecensa (alectinib) label expansion in ALK-positive NSCLC in multiple countries. Roche reported that Flatiron's real-world data "accelerated access for patients by more than a year" in over 20 countries by providing regulators with control arm data on local standard-of-care performance, enabling faster reimbursement decisions without conducting additional RCTs in rare biomarker populations.
What didn't work initially: Data completeness varied significantly across practices. Custom algorithms were required to handle missing data, loss-to-follow-up bias, and differences in treatment patterns. Regulatory submissions required extensive sensitivity analyses to address FDA and international regulators' questions about comparability between trial populations and real-world cohorts.
Lesson: Real-world data is never "plug and play." Budget substantial time and resources for data curation, bias assessment methodology, and iterative regulatory dialogue. Building regulatory confidence in RWE approaches requires methodological rigor and willingness to conduct extensive validation analyses.
Janssen Heartline: Large-scale digital engagement
What they did: Launched a decentralized, app-based cardiovascular study using iPhone and Apple Watch technology to detect atrial fibrillation in adults aged 65+. Participants engaged entirely remotely through the Heartline app, with no required site visits. The study enrolled over 34,000 participants across the United States, including representation from rural and geographically diverse areas.
Results: One of the largest decentralized cardiovascular studies executed to date. The trial demonstrated sustained high participant adherence through 2-year follow-up, generating evidence on wearable-based AFib detection in a real-world Medicare population. The study successfully recruited a higher percentage of women than typical cardiology trials and achieved notable geographic diversity.
What didn't work initially: Participant onboarding proved more complex than anticipated, with app usability issues contributing to early dropout. The study required mid-course UX redesign to improve the participant experience. Despite targeting 150,000+ participants, actual enrollment reached approximately 34,000, highlighting challenges in converting app downloads (~300,000) to completed study enrollment.
Lesson: Consumer-grade technology doesn't automatically translate to research-grade data capture. The gap between download intent and study completion requires thoughtful design of onboarding flows, ongoing engagement strategies, and willingness to iterate on user experience during execution. Pilot rigorously before setting enrollment targets.
Implementing the future of clinical research: continuous, connected, and predictive
The Honest ROI Conversation
Before diving into implementation, let's address the question every CFO asks: what does this cost, and what's the return?
For a mid-to-large pharmaceutical portfolio, we expect $18-43M over 24 months for enterprise-wide transformation. This includes platform integration and data architecture ($8-20M), operational redesign ($3-8M), structured pilots ($5-10M incremental), and change management ($2-5M, consistently underestimated).
The returns are substantial if you execute systematically. We expect 15-25% reductions in phase II/III timelines (6-12 months per program), 20-30% faster enrollment, 10-15% lower late-stage attrition, and 20-30% portfolio capacity increases.
For portfolios spending $800M-1.5B annually on clinical development, this means: $80-150M in avoided costs, 1-2 additional approvals per year, and 12-18 months earlier market entry for key assets. In blockbuster categories, that time advantage represents $2-5B in peak sales differential.
Break-even: 18-24 months. But these returns only materialize through full transformation, not endless pilots.
Pilot-only strategies rarely generate measurable ROI. They create conference presentations but don't change portfolio-level cycle times or increase program capacity. The difference between pilots and transformation is execution discipline. It's the willingness to deprecate legacy systems, retrain functions, and hold executives accountable for scaling what works.
Which brings us to what operationalizing innovation actually requires. Here's what the roadmap looks like:
Phase 1: Create enterprise visibility (6-12 months)
Before you can optimize, you need to see what you have. Most R&D organizations lack unified visibility across their clinical portfolio.

Exhibit 5: R&D performance tracking inside ITONICS
What this means operationally:
-
Unified clinical portfolio dashboard showing all active and planned studies, enrollment status, milestone risk, and resource allocation
-
Standardized taxonomy across therapeutic areas (you'd be surprised how many organizations can't consistently define "study start" or "first patient in")
-
Cross-functional access: regulatory, medical affairs, commercial, and finance viewing the same data
-
Integration with financial systems to track spend against milestones in real time
Why this is harder than it sounds: Data lives in CTMS, project management tools, spreadsheets, and people's heads. Reconciling this requires data governance, not just technology. Expect 6 months of organizational change management.
ROI: Portfolio visibility alone typically surfaces 15-20% of programs that should be re-prioritized, paused, or killed. This redirection of capital often pays for the entire platform investment.
Phase 2: Standardize decision frameworks (concurrent with Phase 1)
Clinical trials fail when approval criteria are implicit and political. You need explicit, transparent frameworks for go/no-go decisions.
/Still%20images/Radar%20Mockups%202025/capabilities-collaboration-clustering-evaluating-viewing.webp?width=2160&height=1350&name=capabilities-collaboration-clustering-evaluating-viewing.webp)
Exhibit 6: Collaborative evaluation inside ITONICS
What this means operationally:
-
Stage gate and readiness criteria that include not just scientific endpoints, but operational feasibility, competitive positioning, and portfolio fit
-
Pre-specified decision rules for adaptive trials (Bayesian stopping boundaries, futility thresholds) agreed upon before study start
-
Regulatory strategy mapped to portfolio priorities, not individual assets
-
Resource allocation models that prioritize based on risk-adjusted value, not legacy commitments
Why this matters: Organizations that can transparently show why they made portfolio decisions (vs. explaining them retroactively) build institutional confidence in new approaches.
Phase 3: Pilot + scale simultaneously (12-24 months)
The traditional model (pilot, evaluate, then scale) is too slow. Leading organizations are running structured pilots while building the infrastructure to scale successes immediately.
What this looks like:
-
3-5 pilots across different therapeutic areas and phases, each testing a specific hypothesis (decentralization in rare disease, AI-driven site selection in oncology, digital endpoints in CNS)
-
Central PMO tracking learnings in real-time, not waiting for end-of-study reports
-
SOPs drafted in parallel with pilots, not after
-
Training programs designed based on early pilot challenges, ready to deploy when pilots succeed
Example: When a top-10 pharma piloted decentralized trials in dermatology, they simultaneously drafted enterprise DCT SOPs, negotiated home health contracts in top enrollment geographies, and trained 50 CRAs on remote monitoring. When the pilot succeeded, they scaled to 8 programs within 6 months - not 18.
/Still%20images/Kanban%20Board%20Mockups%202025/portfolio-govern-project-boards-2025.webp?width=2160&height=1350&name=portfolio-govern-project-boards-2025.webp)
Exhibit 7: Phase-gate boards showing all initiatives inside ITONICS
Phase 4: Measure what matters (ongoing)
Traditional clinical metrics don't capture value enough. You need new KPIs:
Portfolio-level metrics:
-
Median time from FIH to BLA submission (by therapeutic area)
-
Cost per approved indication
-
Portfolio NPV adjusted for probability of technical and regulatory success
-
Evidence generation ROI: cost per meaningful clinical outcome demonstrated
Operational metrics:
-
Enrollment velocity relative to forecast (by site model type)
-
Protocol amendment rate (adaptive trials should have fewer amendments, not more)
-
Screen failure rates (are your inclusion/exclusion criteria too narrow?)
-
Dropout rates by trial design feature (quantify patient burden impact)
Innovation-specific metrics:
-
Time from pilot success to portfolio-wide adoption
-
Reuse rate of validated digital endpoints across programs
-
Regulatory precedent leverage (how often do earlier FDA agreements accelerate subsequent programs?)
Where to start with ITONICS, the operating system for new treatment development
Clinical and R&D leaders need infrastructure that connects studies, aligns priorities, and enables evidence-based decision-making across the development lifecycle.
/Still%20images/Roadmap%20Mockups%202025/portfolio-visualize-critical-paths-2025.webp?width=2160&height=1350&name=portfolio-visualize-critical-paths-2025.webp)
Exhibit 8: ITONICS roadmap visualizing critical paths
For R&D leaders beginning the transformation, ITONICS offers a starting point: visibility into what you have, clarity on gaps, and structure for prioritizing which innovations to pursue first. It doesn't replace clinical systems like CTMS or EDC. It provides the strategic layer connecting individual studies to portfolio objectives.
Unified portfolio visibility: Centralize active and planned studies, surfacing dependencies, redundancies, and resource constraints. This visibility typically reveals 15-20% of programs that should be re-prioritized, often funding the platform investment through better capital allocation.
Dynamic roadmaps: Display milestones, interdependencies, and risk levels across your portfolio. Adjust plans as new data or technologies emerge without losing institutional alignment.
Technology scouting and analytics: Automated scanning for emerging technologies (digital biomarkers, AI trial tools) combined with structured evaluation frameworks. Prioritize opportunities based on strategic fit, feasibility, and risk.



